
Your doctor mentioned you might be “entering perimenopause.”
You assumed that meant hot flashes during meetings and maybe some mood swings — not these frustrating 2–3 AM wake-ups that leave you exhausted all day.
Here’s the reality:
40–60% of women in perimenopause experience significant sleep disturbances (Baker et al., 2015).
What surprises most women is the pattern. You may fall asleep normally — but staying asleep becomes the real struggle. You wake up multiple times during the night, sometimes drenched in sweat, other times wide awake with racing thoughts about things that don’t even matter in daylight.
This article explains:
- The science behind perimenopause-related sleep disruption
- Why it often starts before obvious cycle changes
- The most evidence-based strategies to improve sleep
What Is Perimenopause — and Why Does It Hijack Sleep?
Perimenopause is the natural transition phase leading to menopause. During this time, ovarian hormone production becomes erratic, especially estrogen and progesterone.
This hormonal fluctuation can cause:
- Irregular periods
- Hot flashes and night sweats
- Vaginal dryness
- Mood swings
- Sleep disturbances
Perimenopause typically begins in a woman’s mid-to-late 40s but can start in the 30s for some women (Delamater & Santoro, 2018).
The Link Between Perimenopause and Sleep Disorders
Research shows perimenopausal women have 29% higher odds of sleep disturbance compared to premenopausal women (Kravitz et al., 2011).
This is more than just feeling tired. Chronic sleep disruption during the menopausal transition is associated with:
- Increased cardiovascular risk
- Cognitive changes
- Reduced quality of life
Common Sleep Issues During Perimenopause
- Sleep maintenance insomnia (difficulty staying asleep)
- Frequent nighttime awakenings
- Early morning waking
- Non-restorative sleep
Importantly, sleep changes often begin before noticeable menstrual irregularities. Hormonal shifts affect brain chemistry and thermoregulation long before they visibly alter cycles.
Why Sleep Gets Disrupted During Perimenopause
1. Hormones Are on a Roller Coaster
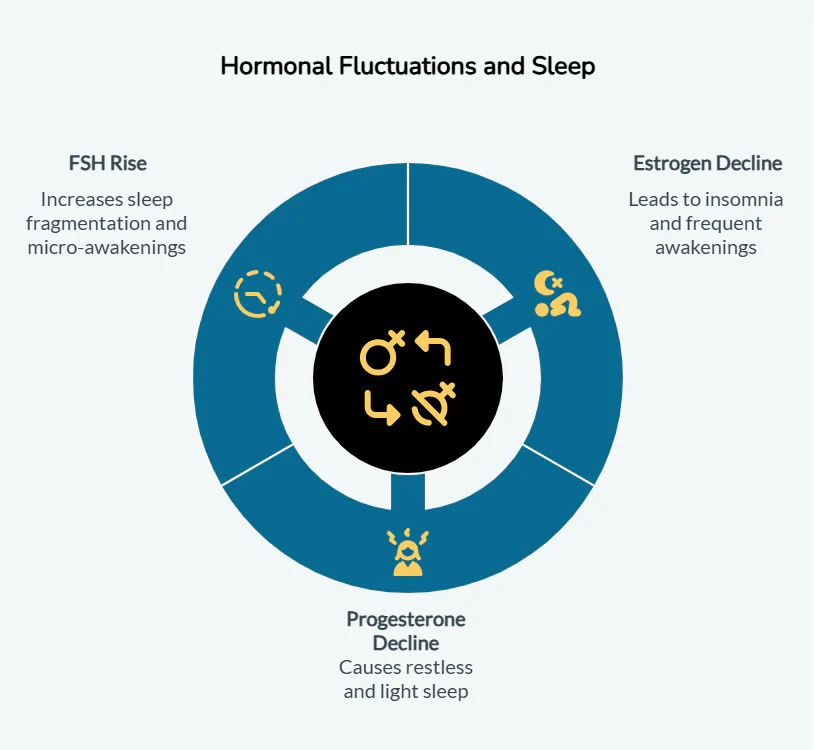
Estrogen and progesterone are powerful sleep regulators.
Estrogen
Estrogen interacts with neurotransmitters like serotonin and melatonin. Declining estrogen levels are linked to difficulty falling and staying asleep (Brown & Gervais, 2020).
Progesterone
Progesterone acts as a natural sedative by enhancing GABA activity. It also helps lower nighttime cortisol levels (Andersen et al., 2006).
FSH and Sleep Fragmentation
As ovarian function declines, follicle-stimulating hormone (FSH) rises. Data from the Study of Women’s Health Across the Nation (SWAN) shows rising FSH correlates with increased sleep fragmentation (Baker et al., 2018).
2. Vasomotor Symptoms Wake You Up
Hot flashes and night sweats affect 75–80% of perimenopausal women (Aminimoghaddam & Abolghasem, 2019).
Fluctuating estrogen disrupts hypothalamic temperature regulation, narrowing the thermoneutral zone. The body overreacts to minor temperature changes — triggering sweating and flushing that wake you repeatedly.
Even if you don’t remember waking, sleep studies show increased nighttime brain arousal.
3. The Mood–Sleep Connection
Hormonal instability also increases risk for anxiety and depression.
A 2025 meta-analysis found depression carries an odds ratio of 2.73 for sleep disorders in perimenopausal women (Zeng et al., 2025).
Chronic stress and anxiety:
- Keep the nervous system hyperaroused
- Disrupt sleep architecture
- Reduce sleep efficiency
Sleep and mood influence each other — treating one often improves the other.
When to See a Doctor
Talk to your provider if you experience:
- Loud snoring or gasping (possible sleep apnea)
- Morning headaches with exhaustion
- Daytime sleepiness affecting daily life
- Chronic insomnia (3+ nights/week for 3+ months)
- Persistent low mood or anxiety
The risk of obstructive sleep apnea increases significantly after menopause.
Evidence-Based Ways to Improve Sleep During Perimenopause
1. Cognitive Behavioral Therapy for Insomnia (CBT-I)
CBT-I is the gold standard first-line treatment for chronic insomnia.
Studies show:
- Telephone-delivered CBT-I reduced insomnia in perimenopausal women (McCurry et al., 2016)
- 55% of postmenopausal women achieved remission at 6 months (Drake et al., 2018)
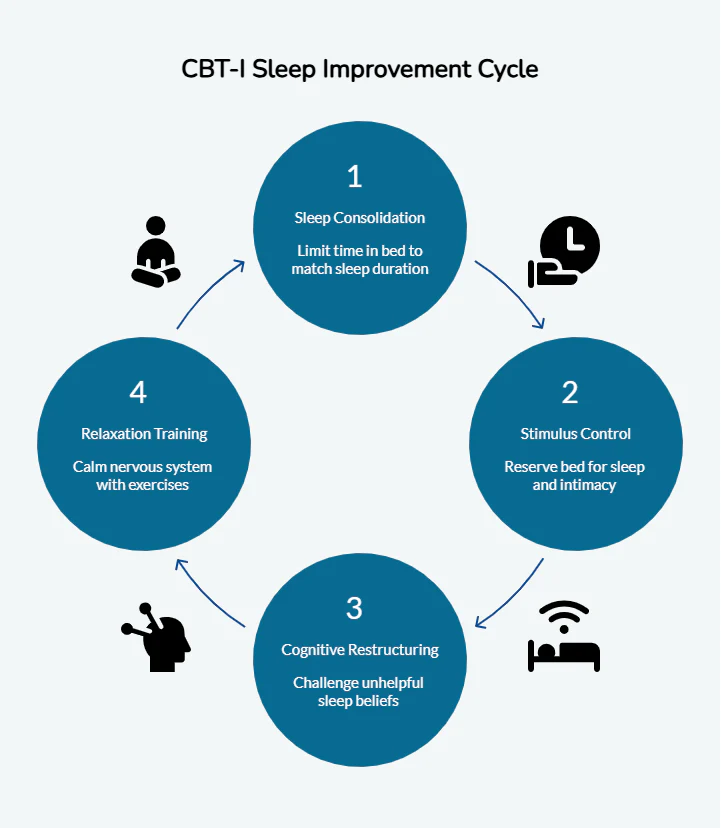
What Happens During CBT-I?
- Sleep consolidation: Limiting time in bed to match actual sleep duration
- Stimulus control: Bed reserved only for sleep and intimacy
- Cognitive restructuring: Challenging catastrophic thoughts
- Relaxation training: Breathwork, progressive muscle relaxation
Unlike sleeping pills, CBT-I addresses root causes without dependency.
2. Take Temperature Regulation Seriously
Optimal bedroom temperature: 60–67°F (16–19°C).
Evidence-based strategies:
- Use moisture-wicking fabrics (bamboo, Tencel)
- Layer bedding
- Cooling mattress pads (Avis et al., 2022)
- Cool shower 60–90 minutes before bed (Neilson, 2019)
- Avoid blue light 1–2 hours before sleep
- Use blackout curtains or eye masks
Small environmental adjustments can significantly reduce awakenings.
3. Hormone Replacement Therapy (HRT) — When Appropriate
For moderate to severe vasomotor symptoms, HRT is the most effective treatment.
A 2022 meta-analysis (Pan et al.) found:
- Improved self-reported sleep quality
- Transdermal estradiol more effective than oral estrogen
- Benefits typically emerge after several months
Who Should Consider HRT?
- Women with severe night sweats
- Those within 10 years of menopause onset
Who Should Avoid HRT?
- History of hormone-sensitive cancers
- Blood clot or stroke history
- Unexplained vaginal bleeding
- Active liver disease
Micronized progesterone may offer additional sleep benefits compared to synthetic progestins.
Always consult a knowledgeable healthcare provider for individualized risk assessment.
4. Magnesium Supplementation
Magnesium regulates:
- GABA activity
- Melatonin production
- Cortisol levels
Supplementation has shown improvements in:
- Sleep onset
- Total sleep time
- Sleep efficiency
- Melatonin levels
Magnesium glycinate is often better tolerated.
However:
- Avoid excessive doses
- Maintain spacing from certain medications
- Supplement only if intake is inadequate or deficiency exists
5. Rule Out Underlying Conditions
Perimenopausal sleep disruption is multifactorial.
Screen for:
- Sleep apnea
- Mood disorders
- Iron deficiency
- Thyroid imbalance
Treating underlying issues often restores sleep stability.
6. Maintain a Healthy Lifestyle
Lifestyle remains foundational:
- Regular exercise
- Yoga and relaxation techniques
- Balanced nutrition
- Stress management
These support nervous system regulation and improve sleep quality.
Final Thoughts
Sleep disruption during perimenopause is a physiological response to real hormonal and neurological shifts. It is not a personal failure or simply “stress.”
One-size-fits-all solutions rarely work because the underlying drivers vary between individuals.
Instead of cycling through random supplements:
- Identify your primary disruption (hormonal, thermal, psychological, or medical)
- Target interventions strategically
- Seek care from providers who understand perimenopausal physiology
Quality sleep is still possible — but it requires precision, not guesswork.
Leave a Reply