
Testing, Treatment & Prevention — Backed by Research
Feeling exhausted even after a full night’s sleep?
Struggling with brain fog, hair shedding, or shortness of breath during normal activity?
You’re not alone.
According to the Centers for Disease Control and Prevention (CDC), iron deficiency is one of the most common nutrient deficiencies among women of reproductive age in the United States. Globally, it remains the leading cause of anemia.
And yet — it’s often overlooked.
Many women are told they’re “just stressed,” “burned out,” or “hormonal.” But sometimes, the real issue is much simpler: your body doesn’t have enough iron to carry oxygen efficiently.
This guide will help you understand:
- What iron deficiency really is
- How to test for it properly
- What research says about treatment
- How to prevent it long term
What Is Iron Deficiency Anemia?
Iron is essential for producing hemoglobin, the protein in red blood cells that carries oxygen throughout your body.
Without enough iron:
- Your cells receive less oxygen
- Your energy drops
- Your brain function slows
- Your heart works harder
The National Institutes of Health (NIH) confirms that iron deficiency develops gradually and often progresses through stages before anemia is diagnosed.
The 3 Stages of Iron Depletion
Stage 1: Low Iron Stores (Low Ferritin)
Ferritin drops, but hemoglobin is still normal.
Symptoms may be subtle — mild fatigue or hair thinning.
Stage 2: Iron Deficiency Without Anemia
Red blood cells become smaller and paler (microcytic, hypochromic).
Ferritin is low. Hemoglobin may still appear “normal.”
Brain fog, restless legs, and reduced stamina are common.
Stage 3: Iron Deficiency Anemia (IDA)
Both ferritin and hemoglobin are low.
Classic symptoms appear:
- Severe fatigue
- Pale skin
- Dizziness
- Shortness of breath
- Brittle or spoon-shaped nails
(Source: NIH Office of Dietary Supplements; American Society of Hematology)
Ferritin vs. Transferrin — Why Both Matter
Many U.S. clinicians now emphasize looking beyond hemoglobin alone.
Ferritin = Your stored iron
Low ferritin means depleted reserves.
Transferrin = Iron transport protein
When iron is low, transferrin rises as your body tries to compensate.
According to the American Society of Hematology (ASH):
- Ferritin <30 µg/L strongly suggests iron deficiency
- Transferrin saturation (TSAT) <20% supports the diagnosis
Importantly, ferritin can appear falsely normal during inflammation — which is why checking CRP (C-reactive protein) can improve accuracy.
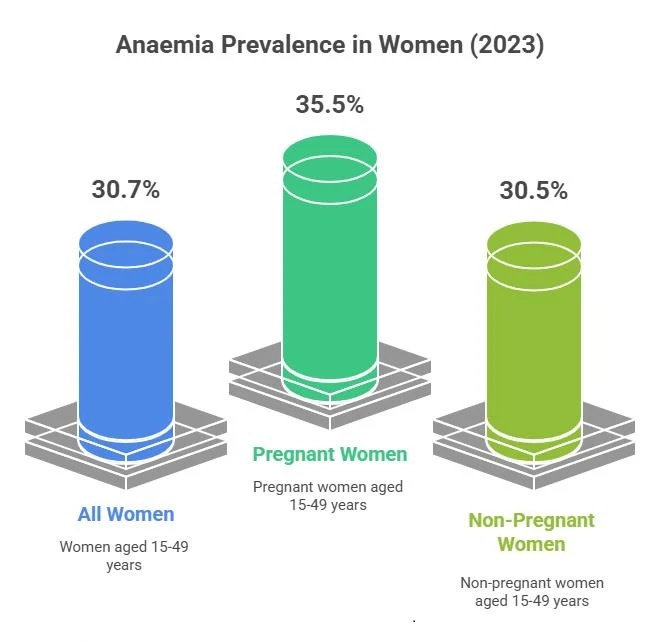
Why Women in the U.S. Are at Higher Risk
Iron deficiency disproportionately affects women — especially between ages 15–49.
1. Menstrual Blood Loss
The American College of Obstetricians and Gynecologists (ACOG) reports that heavy menstrual bleeding is one of the leading causes of iron deficiency in U.S. women.
Even “normal” cycles cause iron loss monthly.
2. Pregnancy & Postpartum
The CDC recommends 27 mg of iron daily during pregnancy due to increased blood volume and fetal demands.
Many women enter pregnancy already low.
3. Diet Trends
Plant-based diets are increasingly popular in the U.S. Non-heme iron (from plants) is less bioavailable than heme iron from meat.
Absorption rates:
- Heme iron: 15–35%
- Non-heme iron: 2–20%
(Source: NIH Office of Dietary Supplements)
4. Hidden Medical Causes
Conditions common in the U.S. such as:
- Celiac disease
- H. pylori infection
- Bariatric surgery history
- Chronic NSAID use
can impair absorption or increase blood loss.
Early Warning Signs Women Often Ignore
Iron deficiency rarely happens overnight. It builds slowly.
Common early symptoms:
- Persistent fatigue (even after rest)
- Brain fog
- Hair thinning
- Pale skin
- Shortness of breath
- Cold intolerance
- Restless legs
- Ice cravings (pica)
Research in JAMA and The American Journal of Clinical Nutrition shows that even mild iron deficiency (without anemia) can impair cognitive performance and mood.
If your energy is consistently below a 7 out of 10 — it’s worth investigating.
Proper Testing: What to Ask Your Doctor For
A basic CBC is not enough.
According to the American Society of Hematology and recent consensus reviews, an ideal iron panel includes:
- CBC
- Serum ferritin
- Serum iron
- TIBC
- Transferrin saturation (TSAT)
- CRP (if inflammation suspected)
Modern Ferritin Perspective
Historically:
Ferritin <15 µg/L = deficiency
Now many U.S. clinicians consider:
Ferritin <30 µg/L = iron deficiency
Ferritin <50 µg/L = may cause symptoms in women
(Referenced in hematology consensus reviews and Lancet publications)
What’s New in Iron Research?
1. Alternate-Day Dosing (Lancet Haematology)
A 2017–2023 series of studies in The Lancet Haematology showed that:
Taking iron every other day
→ improves absorption
→ reduces constipation
→ lowers nausea
Why? Because iron increases hepcidin, the hormone that temporarily blocks absorption. Spacing doses improves efficiency.
2. Smarter Supplement Forms
Traditional iron (ferrous sulfate) works — but causes GI side effects in up to 40% of women.
Newer options:
- Iron bis-glycinate
- Liposomal iron
- Sucrosomial iron
Studies in Nutrients and European Review for Medical and Pharmacological Sciences suggest improved tolerability and comparable efficacy.
3. IV Iron Is Safer Now
Modern IV iron (ferric carboxymaltose, ferric derisomaltose) has significantly lower risk of severe reactions compared to older formulations.
According to the American Society of Hematology, IV iron is appropriate when:
- Oral iron fails
- Absorption is impaired
- Rapid correction is needed
Many women report improved energy within 1–2 weeks.
Food First: Practical U.S.-Friendly Prevention Tips
Best Heme Sources (Highly Absorbable)
- Lean beef
- Turkey
- Chicken thighs
- Salmon
Strong Plant Sources
- Lentils
- Spinach
- Black beans
- Tofu
- Pumpkin seeds
- Fortified cereals
Boost absorption by:
- Pairing with vitamin C (bell peppers, citrus, tomatoes)
- Avoiding coffee/tea around iron-rich meals
The NIH confirms vitamin C can double non-heme iron absorption.
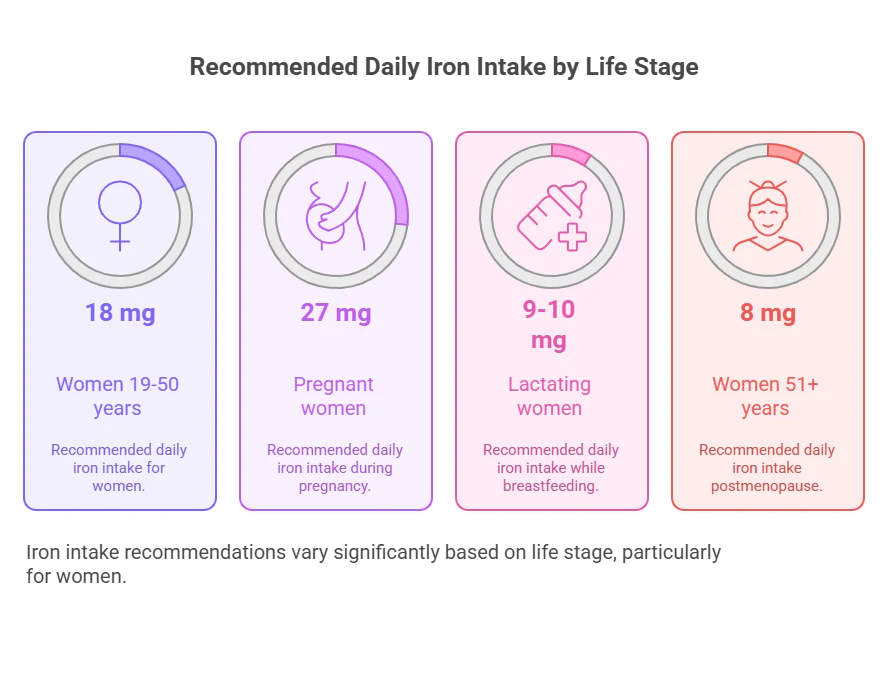
Recommended Daily Iron Intake (NIH Guidelines)
- Women 19–50 years: 18 mg/day
- Pregnant women: 27 mg/day
- Women 51+: 8 mg/day
(Source: NIH Office of Dietary Supplements)
Treatment Strategy: A Research-Based Plan
Step 1: Oral Iron
Typical dosing:
40–65 mg elemental iron
Often every other day
Recheck labs after 8–12 weeks.
Step 2: IV Iron (If Needed)
Used when:
- Severe deficiency
- Pregnancy complications
- Malabsorption
- Intolerance to oral iron
Step 3: Maintenance
Continue low-dose iron or iron-rich diet for 3–6 months after hemoglobin normalizes to replenish ferritin stores.
Key Takeaways
- Don’t rely on hemoglobin alone.
- Ferritin matters — aim for at least 30–50 µg/L.
- Heavy periods are a major cause.
- Alternate-day dosing improves absorption.
- Vitamin C enhances uptake.
- IV iron is a safe modern option when necessary.
- Recheck labs — don’t assume correction after one bottle of supplements.
Final Thoughts: Restoring Iron, Restoring Energy
Iron deficiency is not just about feeling tired.
It affects:
- Focus
- Mood
- Exercise capacity
- Immune function
- Cardiovascular strain
If you’ve been dismissed or told “everything looks normal,” ask to see your ferritin.
Advocating for yourself is not overreacting — it’s informed healthcare.
With proper testing, smart supplementation, and consistency, most women recover fully and feel dramatically better.
Leave a Reply